Antistreptolysin O (ASO/ASLO)
- ASLO/ASO latex kit test: an indirect agglutination kit for the detection of anti-streptolysin-O in human serum using latex particles coated with streptolysing-O. 

ASO titer is adviced for the diagnosis of post infectious glomerulonephritis, scarlet fever, streptococcus infections and others. The Streptolysin O is antigenic and cause hemolysis of RBCs. So there is antibody formation (Antistreptolysin-Ab) in the blood.
Anti-Streptolysin O (ASO or ASLO) is the antibody made against streptolysin O, an immunogenic, oxygen-labile hemolytic toxin produced by most strains of group A and many strains of groups C and G streptococci.
In the course of streptococcal infections, the extracellular products of the bacteria act as antigens to which the body responds by producing specific antibodies. Streptolysin O (ASLO) is one of two hemolysins (the other being Streptolysin S) produced by virtually all strains of Streptococcus pyogenes.
Principle:
Patient serum with dilution is mixed with a fixed amount of streptolysin O- Ag and a reaction takes place. Then add Ab-coated RBC. There will be hemolysis in the tube, where streptolysin O is free.
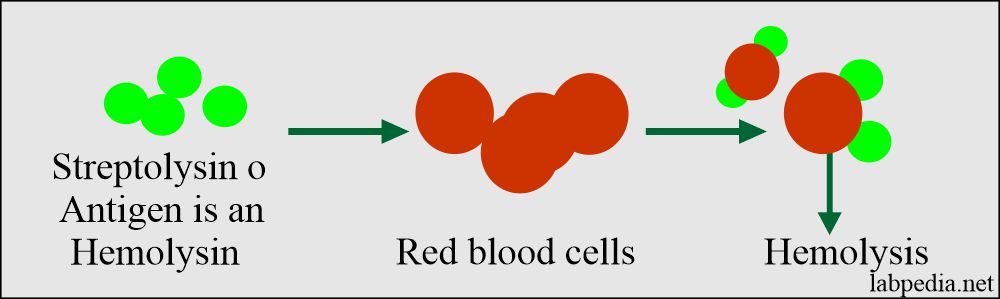
Antistreptolysin (ASO) leading to hemolysis
The result is reciprocal of the highest dilution where hemolysis starts. Units are international units (IU).
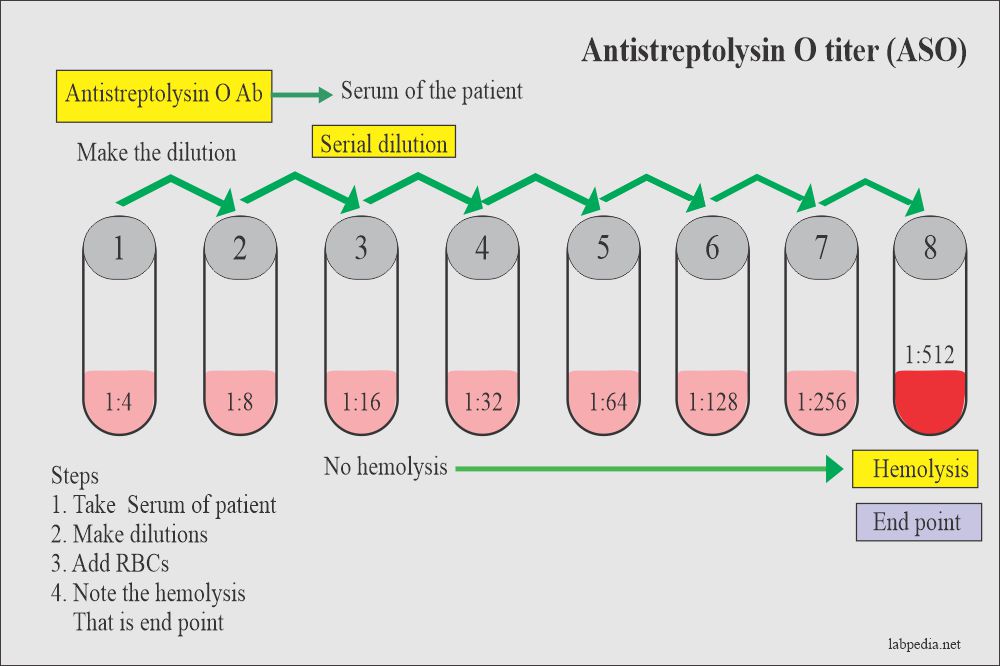
Antistreptolysin (ASO) titer procedure
Normal value: below 200.
Definitive value: 400 or more.
Rising titer from 200-250 is significant.
ASLO-Latex Test: The assay is performed by testing a suspension of latex particles coated with streptolysin O antigen against unknown serum. The presence or absence of visible agglutination indicates the presence or absence of ASLO in the samples tested.
REAGENT COMPOSITION ASLO-Latex Antigen. Suspension of polystyrene latex particles coated with stabilized streptolysin O in a buffered saline solution.
CONTROL + Human serum with an ASLO activity > 200 IU/mL.
CONTROL - Animal serum with an ASLO activity < 100 IU/mL.

Precautions: Components of different human origin have been tested and found to be negative for the presence of antibodies anti-HIV 1+2 and anti-HCV, as well as for HBsAg. Do not allow to contact with skin or mucous membranes.
EXPECTED VALUES: 95% of healthy adults have ASLO titers of 200 IU/mL or less, the highest titers been found in school children with titers up to 250 IU/mL. Since a single ASLO determination does not provide much information unless it is high, titrations at bi-weekly intervals for 4 to 6 weeks of the doubtful cases are advisable to follow the evolution of the disease.
CLINICAL SIGNIFICANCE: Elevated ASLO serum titers occur in response to infection with hemolytic streptococci of Group A, C and G, producers of streptolysin O, an extracellular protein of enzymatic character with strong antigenic properties. Immunochemical assay of these specific antibodies to streptococcal metabolites provide valuable information to establish a diagnosis of streptococcal infections (acute rheumatic fever, glomerulonephritis). ASLO testing has a high diagnostic value on a tentative diagnosis made on the basis of case history and clinical findings.
ANALYTICAL PERFORMANCE: The minimum detectable unit (analytical sensitivity) is of approximately 200 IU/mL (± 50 IU/mL). 

LIMITATIONS OF PROCEDURE: Positive reactions do occur in conditions other than glomerulonephritis, in which the production of ASLO is especially high. In scarlet fever, early and acute periods of rheumatoid arthritis, healthy carriers, complicated and no complicated tonsillitis and various streptococcal infections increased ASLO levels have been found. Biologically false negative reactions can occur in early infections and during the early years of life (from six months to 2 years). The sensitivity of the test may be reduced at low temperatures. The best results are achieved at 15-25ºC. Delays in reading the results may result in over-estimation of the antibody present.
No comments:
Post a Comment